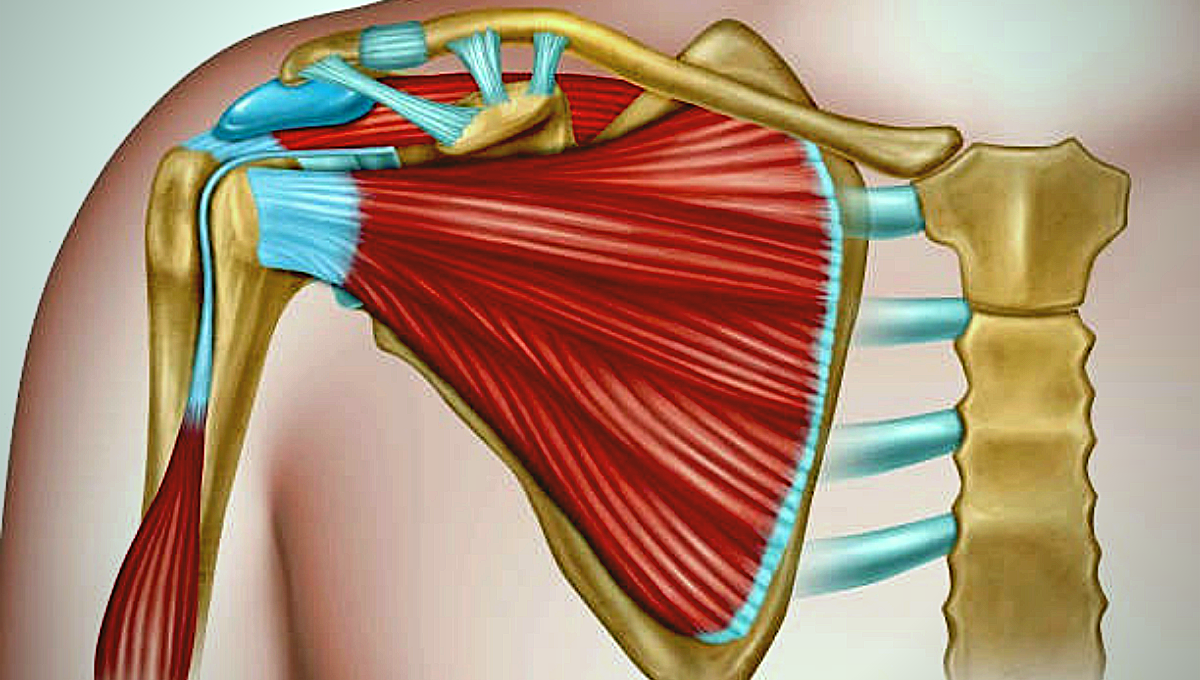
The shoulder or pectoral girdle is made up of bones that connect the upper extremities with the axial skeleton. The question is “What bones make up the shoulder?” In one sentence the answer is “the shoulder complex made up by four bones, namely the humerus, clavicle, shoulder bone (Scapula), and the posterior surface of the ribs”. It is one of the largest and most complex joints in the body.
The joints of the shoulder are Glenohumeral Joint (GH), the Acromioclavicular Joint (AC), the Sternoclavicular Joint (SC), and a “floating joint”, known as the Scapulothoracic joint (ST).
Glenohumeral Joint (GH): The glenohumeral joint (GH) is a genuine synovial ball-and-socket style diarthrodial joint, liable for associating the furthest extremities to the trunk. It is one of the four joints that make up the shoulder complex. The joint is made up of the head of the humerus of the shoulder bone and the glenoid fossa. This joint is considered the most mobile and unstable joint in the human body and is the most commonly dislocated diarthrodial joint.
Acromioclavicular Joint (AC): The acromioclavicular joint or AC joint is one of the four joints that make up the shoulder complex. The Acromioclavicular Joint is a joint formed by the lateral clavicle and the acromion process of the scapula. It is a sliding or flat synovial joint. The AC joint connects the shoulder cap bone to the clavicle and serves as the main joint that suspends the upper extremities of the torso.
Sternoclavicular Joint (SC): The Sternoclavicular Joint (SC joint) is made from the articulation of the medial aspect of the clavicle and therefore the manubrium of the sternum. The Sternoclavicular Joint (SC joint) is that the only true articulation connecting the upper limb to the skeletal structure, which it’s the smallest amount constricted joint within the human body. It’s one among four joints that compose the Shoulder Complex. The Sternoclavicular joint (SC) is usually classified as a plane-style articulation synovial and features a fibrocartilage joint disk. The joint ligament reinforcement is very strong and generally leads to a clavicle fracture prior to SC joint dislocation.
Scapulothoracic joint (ST): The “joint” of the shoulder scapulothoracic (ST) joint is not a true anatomical joint because it does not have the usual joint characteristics (combined by fibers, cartilage, or synovial tissue). It is the joint between the scapula bone and the thorax, which depends on the integrity of the anatomical joints of the acromioclavicular (AC) and the sternum (SC). The sternoclavicular (SC) and acromioclavicular (AC) joints are interdependent with the Scapulothoracic (ST) joint because the scapula is attached by its acromion process to the lateral end of the clavicle & through the acromioclavicular (AC) joint; the clavicle, in turn, is attached to the skeletal structure at the manubrium of the sternum through the Scapulothoracic (SC) joint. Any movement of the shoulder bone (Scapula) at the sternum must end in movement at the acromioclavicular (AC) joint, the SC joint, or both.; that’s, the functional ST joint is a component of a real ring with the acromioclavicular (AC) and Scapulothoracic (SC) joints and therefore the thorax.
What bones make up the Shoulder
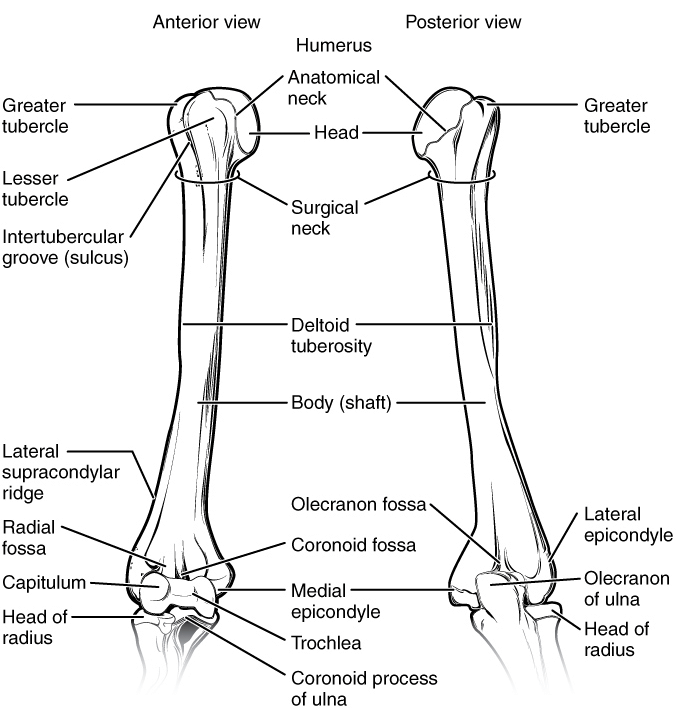
Humerus
The humerus is a long bone that forms a joint between the proximal end (with the cap bone) and the ulnar joint of the humerus and the radial joint of the humerus (with the ulna and radius bones, respectively). The head of the humerus is semicircular, towards the head, in the middle, slightly back, and covered with smooth hyaline cartilage. The head and glenoid socket of the shoulder cap are articulated, and the shoulder lens fossa is a fossa that is much smaller in diameter than the humeral head.
The direction of the plane of the humeral head and the glenoid fossa presents a ball-and-socket relationship, especially compared to the ball-and-socket coxa femoral joint, allowing the shoulder to have a greater range of motion. The role of the glenoid cavity is further deepened by the labrum, which is a fibrocartilage structure composed of the fusion of ligaments and capsular attachments.
The anatomical neck of the humerus is located at the distal end of the articular head of the humerus. The anatomical neck of the humerus is obliquely directed upward and is represented by a narrow groove separating the top of the humerus from the lesser and greater tubercles.
The anatomical neck is that the attachment site of the articular capsule of the glenohumeral joint and therefore the corresponding glenohumeral ligaments. Greater and lesser tubercles are two prominent features of the humerus. The greater tubercle is positioned lateral to the top of the humerus and the lesser tubercle is medially located on the bone.
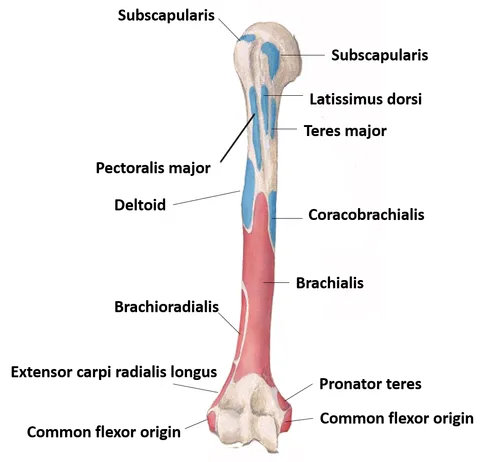
The greater tubercle provides a site of insertion to the –
- Supraspinatus,
- Infraspinatus and
- Teresminor muscle.
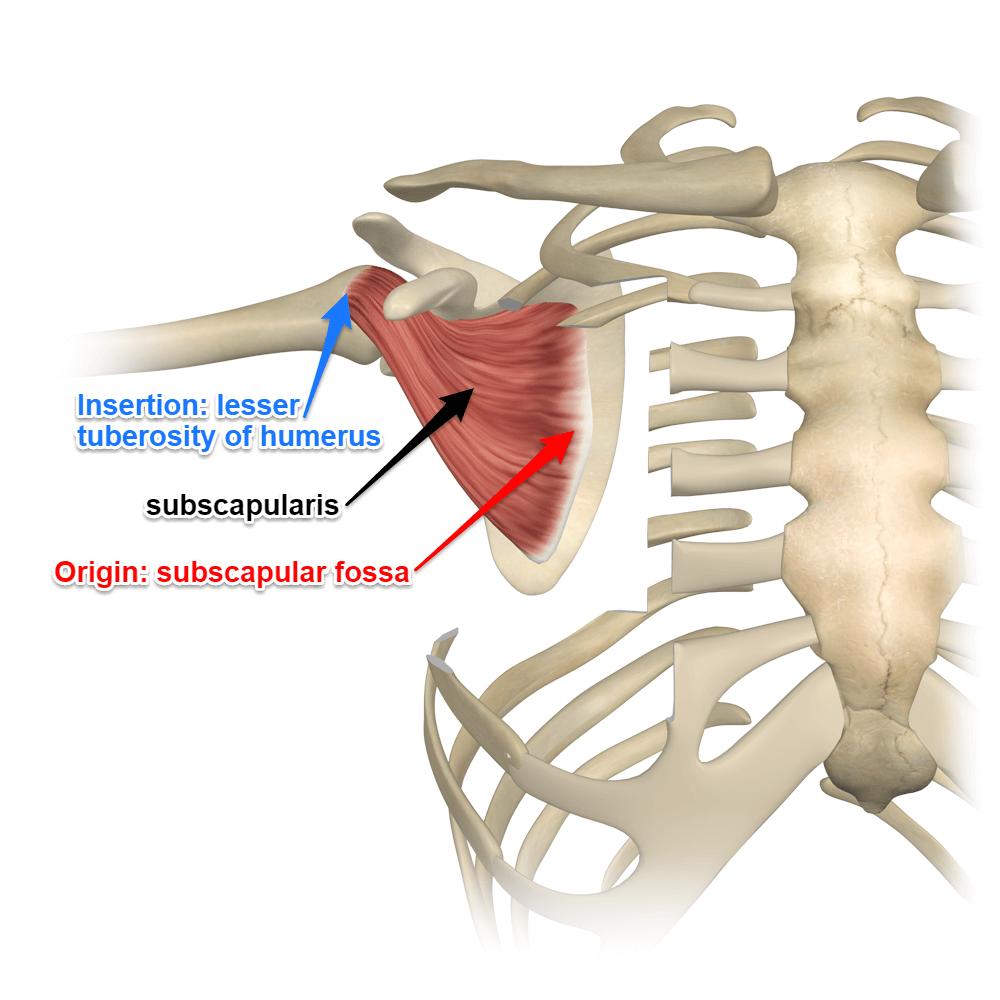
The lesser tubercle provides the insertion of the tendon of the –
- Subscapularisand lies medially and inferior to the top of the humerus.
The greater and lesser tubercles are separated by the bicipital groove during which the long head of the musculus biceps brachialis.
The pectoral ridge extends from the greater tubercle along the medial edge of the bone and is that the insertion site of the musculus pectoralis major. The deltoid ridge extends from the greater tubercle along the lateral edge of the humerus and is that the broad insertion site for the deltoid group. Caudal to the greater and lesser tubercle is that the surgical neck of the humerus. The surgical neck is narrower than the proximal humerus and may be a common site of fractures.
Clavicle
The clavicle contributes to the anterior and superior aspects of the glenohumeral articulation. The clavicle is an elongated, S-shaped bone that lies horizontally on the anterior aspect of the chest wall and articulates medially with the manubrium sterni, and laterally with the acromion of the scapula.
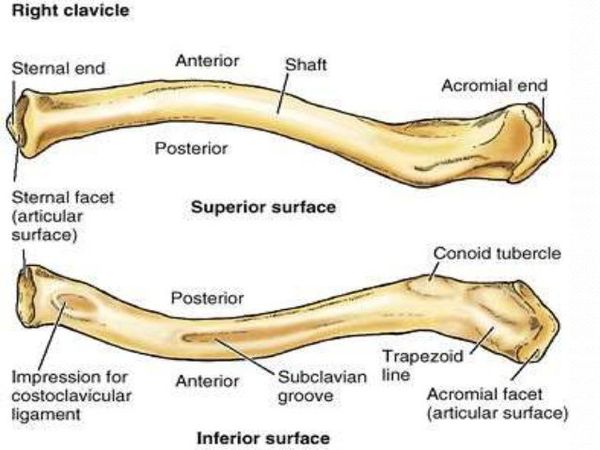
The clavicle has been compared to a “crank” because it contains double curves several muscles, including the deltoid, the trapezius, and the pectoralis major, have important attachments to the c1avicles.
The lateral aspect of the clavicle, the area that articulates with the acromion of the scapula, is generally concave with a roughened attachment for the acromioclavicular (AC) ligaments. The acromioclavicular (AC) joint is generally oriented laterally and posteriorly, although variations do exist. The superior acromioclavicular (AC) ligaments are better defined and thicker than the inferior acromioclavicular (AC) ligaments and attach in the roughened region of the distal c1avicles. Damage to the joint can lead to a variety of abnormal movements including increased superior excursion and abnormalities in rotation.
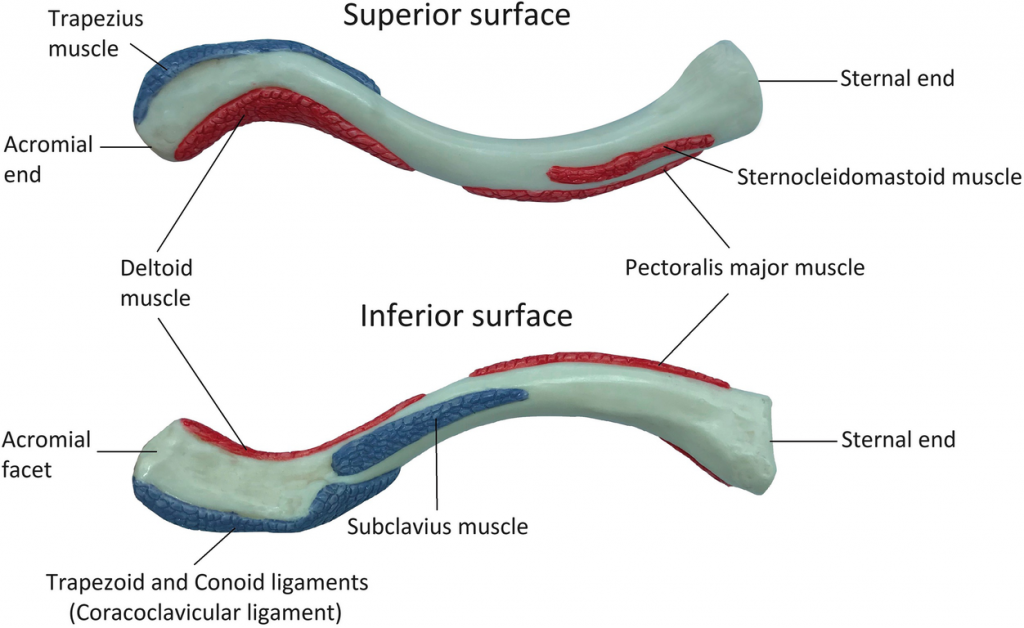
There are six muscles in the clavicle, distributed in the outer (lateral) third or the inner (medial) two-thirds of the bone.
Two muscles are attached to the outer (Lateral) third of the clavicle.
1. The trapezius muscle is attached along the posterior surface of the bone.
2. The deltoid muscle (anterior portion of the muscle) is attached to the periosteum at the anterior surface of the bone.
There are four muscles are attached to the medial third of the clavicle:
1. The sternocleidomastoid, where the muscular clavicular head of the muscle is attached to the superior surface of the bone.
2. The musculus pectoralis major muscle, which is attached to the anterior surface of the bone.
3. The subclavius muscle, which is attached to a groove found within the middle of the bone’s inferior surface.
4. The sternohyoid muscle, which attaches to the medial end of the clavicle.
Scapula
The scapula forms the posterior and superior aspects of the shoulder glenohumeral articulation. The concave ventral surface of the scapula creates a pseudo articulation with the thorax. The stabilization of the concave surface to the thorax is performed by the complex interaction of several muscles that stabilize the joint during static and dynamic actions. The dorsal surface is divided into superior and inferior sections by the spine of the scapula.
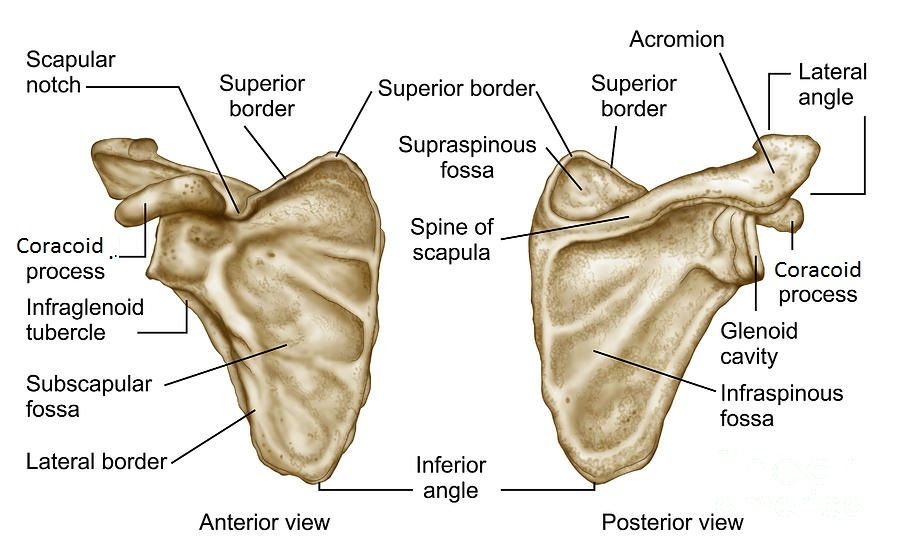
The inferior section houses the origination of the infraspinatus, and teres minor and major, while the superior section is the origination of the supraspinatus. The acromion forms as a projection from the spine of the scapula and overhangs the glenoid cavity. The medial border of the acromion articulates with the lateral aspect of the clavicle and is convex in shape. Studies have suggested that the acromion takes several different shapes that may predispose the individual to impingement-related problems.
Bigliani and Morrison identified three types of acromion shapes based on the grade of the anterior slope at the distal aspect. The third type, which has a hooked slope, is frequently seen in patients with impingement syndrome and rotator cuff tears.
Globe of BlogsReference
- Shoulder
- Shoulder Joint Anatomy
- kenhub.com
- Orthopedic Manual Therapy by CHAD E. COOK, PT, Ph.D., MBA, OCS, COMT